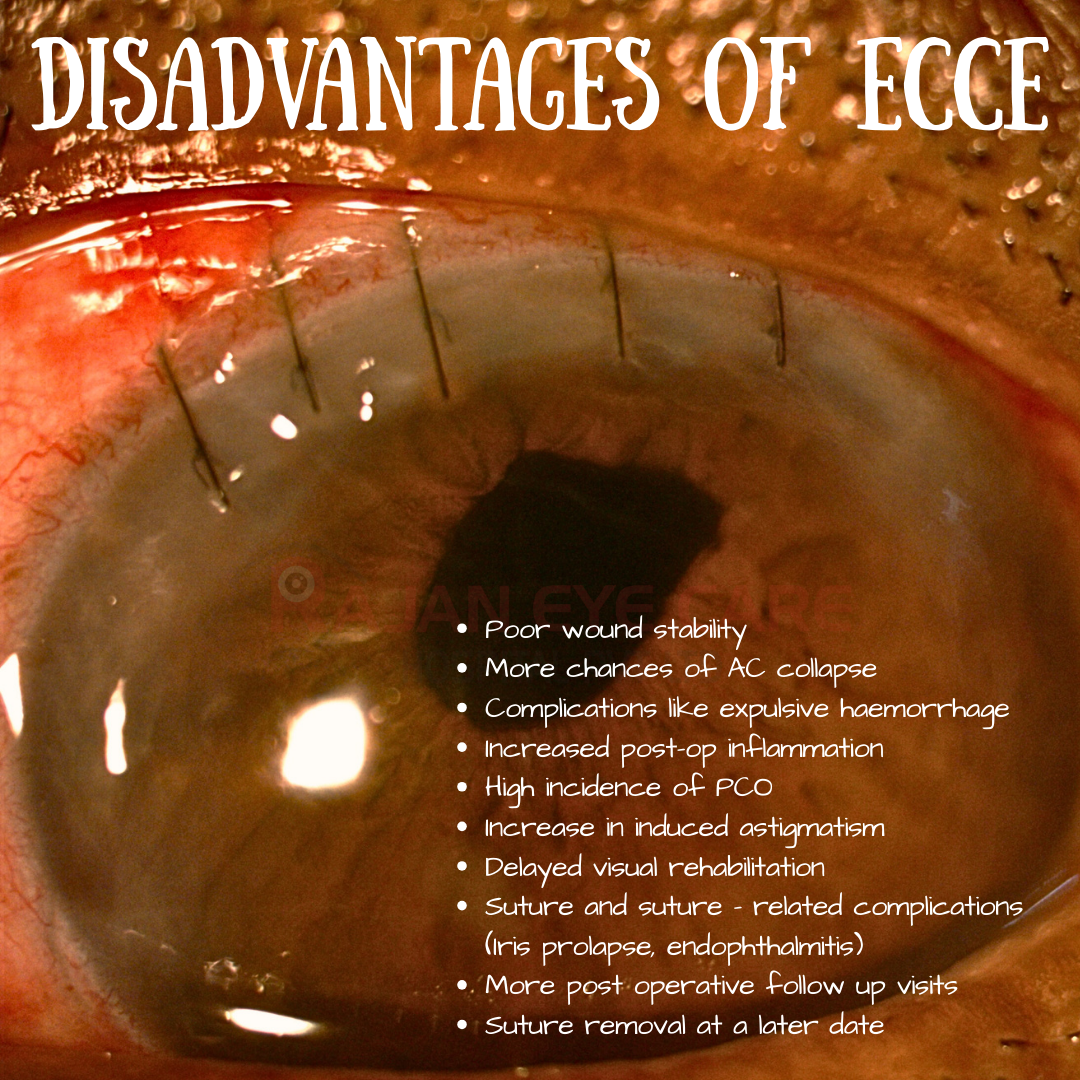
Disadvantages of ECCE
1) Large Incision Size
- Requires a 10–12 mm scleral or corneal incision for nucleus delivery.
- Leads to slower wound healing and higher induced astigmatism.
2) Higher Surgically Induced Astigmatism (SIA)
-Large corneoscleral incision significantly alters corneal curvature.
-Reported SIA after ECCE: ~2–4 D, compared with <1 D in phaco.
3) Slower Visual Rehabilitation
-Because of wound size, patients experience delayed stabilization of refraction and visual acuity compared with phacoemulsification
4) Higher Risk of Wound-Related Complications
-Wound dehiscence, iris prolapse, and infection risk (e.g., endophthalmitis) are higher due to larger wound.
5) Greater Dependence on Sutures
-Sutured closure often needed, which can induce irregular astigmatism, suture-related vascularization, or infection
6) Posterior Capsular Opacification (PCO) Rates
PCO remains a problem after ECCE, though it also occurs with phaco. Some studies suggest slightly higher incidence due to less controlled cortical cleanup.
7) Longer Recovery & Return to Activities
-Post-operative recovery time (functional vision, return to daily tasks) is longer compared with phacoemulsification.
8) Less Suitable for High-Volume Surgery Settings
-Longer surgical and recovery time compared with small-incision cataract surgery (SICS) and phacoemulsification, limiting efficiency in high-volume eye care
www.ophthalmobytes.com
Image from Rajan Eye Care Hospital
#ophthalmology #ophthal #doctor #health #medical #vision #education #optometry #medicalstudent #optometrist #medicine #ophthalmologist #ophthalmo #med #medicaleducation #ophthalmologyresident #ophthalmologyresidency #apaoyo #lens #cataract #cataractsurgery #ecce #extracapsularcataractextraction